Volkan Hanci,1 Fusun Cömert,2 Hilal Ayoğlu,1 Canan Kulah,2 Serhan Yurtlu,1 Işıl Ozkoçak Turan1
1Anesthesiology and Reanimation Department, Medicine Faculty, Zonguldak Karaelmas University, Zonguldak, Turkey; 2Microbiology Department, Medicine Faculty, Zonguldak Karaelmas University, Zonguldak, Turkey
Correspondence: Volkan Hanci, Anesthesiology and Reanimation Department, Medicine Faculty, Zonguldak Karaelmas University, Zonguldak, Turkey. E-mail: vhanci@gmail.com
Key words: atracurium; rocuronium; mivacurium; antimicrobial effect.
Conflict of interest: the author reports no conflicts of interest.
Received for publication: 10 September 2010.
Revision received: 22 December 2010.
Accepted for publication: 22 December 2010.
©Copyright V. Hanci et al., 2011
Licensee PAGEPress, Italy
Drugs and Therapy Studies 2011; 1:e2
doi:10.4081/dts.2011.e2
AbstractSome anaesthetic agents may be contaminated with microorganisms during the process of preparing an infusion. For this reason, it is important to understand the antimicrobial effects of various anaesthetic agents, which have been investigated to some degree in previous studies. However, studies specifically focusing on antibacterial effects of neuromuscular blocking drugs (anaesthetic agents) are very rare. Herein, we analysed the antimicrobial effects of atracurium, rocuronium, and mivacurium, on four different microorganisms. The in vitro antimicrobial activities of atracurium, rocuronium and mivacurium were investigated using the broth microdilution method. The pH of the test solutions was determined using a pH meter. The test microorganisms included Staphylococcus aureus ATCC 29213, Enterococcus fecalis ATCC 29212, Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853. The pH of the test solutions ranged between 7.20 and 7.32. The minimum inhibitory concentrations of atracurium, rocuronium and mivacurium for S. auereus, E. fecalis, E. coli and P. Aeruginosa were all found to be 512 µg/mL. Atracurium, rocuronium and mivacurium inhibit the growth of common intensive care unit pathogens at the same concentration (512 µg.mL-1). Thus, the neuromuscular blocking drugs, atracurium, rocuronium and mivacurium should be administered at a minimum concentration of 512 µg/mL in intensive care units to achieve this antibacterial effect. In our opinion, when used systemically, atracurium, rocuronium and mivacurium do not cause a systemic antibacterial effect. However, their antibacterial effects may be advantageous for inhibiting the spread of bacterial contamination during the preparation of the infusion solutions.
|
Some anaesthetic agents are known to support the growth of microorganisms, while other anaesthetic agents neither support nor inhibit microbial growth. The antibacterial effects of anaesthetic agents may be beneficial for reducing the spread of some types of infections brought about by contaminated compounds that are destined to be delivered into patients.1
Atracurium, rocuronium and mivacurium are neuromuscular blocking agents that are commonly used in intensive care units (ICUs).2,3,4,5 However, to date, only one previous study has focused on the antibacterial effects of atracurium.6
The aim of this study was to evaluate the antimicrobial effects of atracurium, rocuronium and mivacurium on microorganisms that are frequently isolated in our ICU. The test microorganisms chosen were S. aureus American Type Culture Collection (ATCC) 29213, E. fecalis ATCC 29212, E. coli ATCC 25922 and P. aeruginosa ATCC 27853.
The antibacterial activities of atracurium, rocuronium and mivacurium were investigated using the broth microdilution method according to the procedures outlined by the Clinical and Laboratory Standards Institute (CLSI).7
Briefly, each neuromuscular blocking drug was diluted with 0.9% sterile saline to final concentrations of 512 µg/mL, 256 µg/mL, 128 µg/mL, 64 µg/mL, 32 µg/mL, 16 µg/mL, 8 µg/mL, 4 µg/mL, 2 µg/mL, 1 µg/mL and 0.5 µg/mL. For each neuromuscular blocking drug, the pH values of all the dilutions were determined with a pH meter (Mettler MP 220, Toledo, Switzerland). S. aureus ATCC 29213, E. fecalis ATCC 29212, E. coli ATCC 25922 and P. aeruginosa ATCC 27853 were used as control microorganisms. The bacteria [5×105 colony-forming units per millilitre; (CFU/mL)], CAMHB (cation-adjusted Mueller-Hinton broth) and the neuromuscular blocking drugs in the specified concentrations were incubated in the wells on microplates at 35°C for 20 hours. The minimal inhibitory concentrations (MIC) were determined by observing the lowest concentration of the agent that inhibited visible growth of the bacterium. Haze or turbidity in the wells were indicators of bacterial growth.
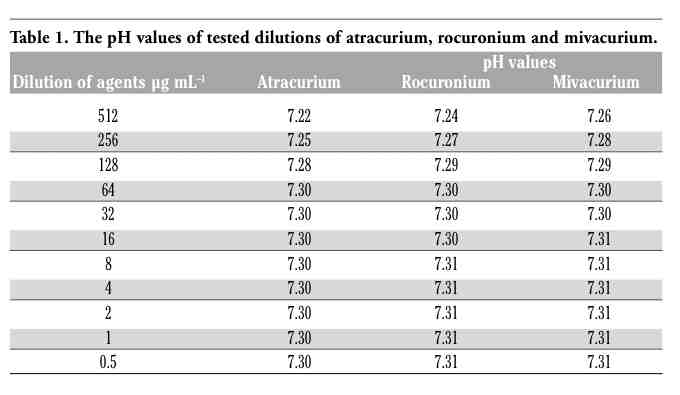
The MIC values of atracurium, rocuronium and mivacurium for S. aureus, E. coli, P. aeruginosa and E. fecalis were all determined to be 512 µg/mL. The pH values of the tested agent solutions are listed in Table 1.
|
Table 1. The pH values of tested dilutions of atracurium, rocuronium and mivacurium. |
In this study, we have found that atracurium, rocuronium and mivacurium have antimicrobial properties with regard to the microorganisms studied. The MIC of the antibacterial neuromuscular blocking drugs were found to be higher in concentration than the plasma concentrations required to produce a 50% inhibition in humans and lower than their recommended clinical use concentrations.
However, some anaesthetic agents may be contaminated by microorganisms during the preparation of an infusion. For this reason, the antimicrobial effects of various anaesthetic agents have been deemed important, and they have been investigated in previous studies. There are also published reports of systemic bacteremias and wound infections involving S. aureus that are linked to the use of intravenous propofol.8 Notably, propofol is known to support the growth of microorganisms.6,9,10,11,12,13,14,15 Yet, previous studies have shown that morphine sulphate, thiopental sodium, fentanyl citrate, dexmedetomidine and midazolam all have antimicrobial effects.1,6,14,15,16 However, studies on the antimicrobial effects of neuromuscular blocking drugs, which are commonly used in ICUs, are very rare.6,11 Graystone et al.6 showed that atracurium demonstrates antibactericidal effects and also reduces fungal growth. However, a study by Durak et al.11 did not support the aforementioned claims of atracurium’s bactericidal effect. In our study, we found that rocuronium, atracurium and mivacurium have antimicrobial properties with respect to the growth of S. aureus, E. coli, P. aeruginosa and E. fecalis.
However, the mechanisms of the antibacterial activity of these three compounds have not been clarified. Several studies have established that the antimicrobial effects of some anaesthetics may depend on their molecular weight, pH and thermodynamic activity.1,6,11 Yet, other studies revealed an interaction between the cytoplasmic membrane and a macromolecule component of the anaesthetic agent.17,18
The bactericidal property of thiopental is thought to be related to its high pH (10.55).19 In several studies, the pH range of midazolam was shown to be responsible for its bacterial inhibitory effect.6,20 Keles et al.16 concluded that the antimicrobial effect of midazolam may be due to the fact that this compound includes HCl as a preservative.
Most pathogenic bacteria prefer a fairly narrow pH range, between 6 to 8, for survival.12,14 However, the growth of S. aureus (ATCC 25923), E. coli (ATCC 25922) or P. aeruginosa (ATCC 27853) were not affected by growth conditions in which the pH was between 5.0 and 8.0.21
In our study, prior to performing the recommended dilution, the pH of the atracurium, rocuronium, and mivacurium solutions were 3.5, 4.1, and 4.0 respectively. However, the diluted drugs all had a pH between the narrow range of 7.20 to 7.32. For this reason, the bactericidal properties of the three compounds in our study could not be due to their pH.
Lipid-based emulsions and preservative-free forms have been shown to support various microorganisms by inhibiting the reticuloendothelial system and thereby suppressing the host’s natural immunity.1,10 Atracurium, rocuronium and mivacurium would then be deemed to be advantageous in that they do not contain lipid-based emulsions. Moreover, the pH values of the undiluted solutions may prevent contamination at clinically relevant concentrations. However, based on a review of the literature, there were no publications addressing the effects of atracurium, rocuronium, and mivacurium on human neutrophil functions, immune function or the inflammatory response.
It is important that strict guidelines regarding the need for sterile equipment and deliverables be adhered to during all procedures performed in the ICU. In some circumstances neuromuscular blocking drugs may be contaminated with microorganisms that can then lead to infections.1 Thus, the antimicrobial effect of neuromuscular blocking drugs in these types of settings is of paramount importance.
The emerging problem of bacterial resistance in the hospital and in the ICU limits the use of antimicrobials because of the risk of the positive selection of resistant bacteria. Although the neuromuscular blocking drugs atracurium, rocuronium and mivacurium are known to have antibacterial effects, these effects are concentration dependant. However, we have found that the working antibacterial concentration of atracurium, rocuronium and mivacurium was higher than the concentration corresponding to a 50% inhibition in their activity (EC50) (454 ng/mL-1, 1008 ng/mL-1 and 130 ng/mL-1, respectively).22,23,24,25
In our opinion, when used systemically, atracurium, rocuronium and mivacurium do not cause a systemic antibacterial effect. However, their antibacterial effects may be sufficient to inhibit contamination during the preparation of the infusion solutions.
As a result, we have shown that atracurium, rocuronium and mivacurium have antibacterial effects on some microorganisms frequently encountered in hospital settings, but when these compounds are administered as an infusion, they should be used at concentrations equal to or greater than 512 µg/mL.
1. Ayoglu H, Kulah C, Turan I. Antimicrobial effects of two anaesthetic agents: dexmedetomidine and midazolam. Anaesth Intensive Care 2008;36:681-4.[PubMed]
2. Reeves ST, Turcasso NM. Nondepolarizing neuromuscular blocking drugs in the intensive care unit: A clinical review. South Med J 1997;90:769-74. [PubMed]
3. Playfor S, Jenkins I, Boyles C, et al.; United Kingdom Paediatric Intensive Care Society Sedation, Analgesia and Neuromuscular Blockade Working Group. Consensus guidelines for sustained neuromuscular blockade in critically ill children. Paediatr Anaesth 2007;17:881-7.[PubMed]
4. Sparr HJ, Wierda JM, Proost JH, et al. Pharmacodynamics and pharmacokinetics of rocuronium in intensive care patients. Br J Anaesth 1997;78:267-73.[PubMed]
5. Farenc C, Lefrant JY, Audran M, Bressolle F. Pharmacokinetic-pharmacodynamic modeling of atracurium in intensive care patients. J Clin Pharmacol 2001;41:44-50.[PubMed]
6. Graystone S, Wells MF, Farrell DJ. Do intensive care drug infusions support microbial growth? Anaesth Intensive Care 1997;25:640-2.[PubMed]
7. Clinical and Laboratory Standards Institute. 2005. Performance standards for antimicrobial susceptibility testing. Document M100-S15. Clinical and Laboratory Standards Institute, Wayne, Pa, USA.
8. Heldmann E, Brown DC, Shofer F. The association of propofol usage with postoperative wound infection rate in clean wounds: a retrospective study. Vet Surg 1999;28:256-9.[PubMed]
9. Henry B, Plante-Jenkins C, Ostrowska K. An outbreak of Serratia marcescens associated with the anesthetic agent propofol. Am J Infect Control 2001;29:312-5.[PubMed]
10. Langevin PB, Gravenstein N, Doyle TJ, et al. Growth of Staphylococcus aureus in diprivan and intralipid: implications on the pathogenesis of infections. Anesthesiology 1999;91:1394-400.[PubMed]
11. Durak P, Karabiber N, Ayoğlu H, et al. Investigation on antibacterial activities of atracurium, lidocaine, propofol, thiopentone, and midazolam. Acta Anaesth Italica 2001;52:39-43.
12. Arduino MJ, Bland LA, McAllister SK, et al. Microbial growth and endotoxin production in the intravenous anesthetic propofol. Infect Control Hosp Epidemiol 1991;12: 535-9.[PubMed]
13. Sosis MB, Braverman B. Growth of Staphyloccoccus aureus in four intravenous anaesthetics. Anesth Analg 1993; 77:766-78.[PubMed]
14. Crowther J, Hrazdil J, Jolly DT, et al. Growth of microorganisms in propofol, thiopental, and a 1:1 mixture of propofol and thiopental. Anesth Analg 1996;82:475-8.[PubMed]
15. Sosis MB, Braverman B, Villaflor E. Propofol, but not thiopental, supports the growth of Candida albicans. Anesth Analg 1995;81:132-4.[Abstract]
16. Keleş GT, Kurutepe S, Tok D, et al. Comparison of antimicrobial effects of dexmedetomidine and etomidate-lipuro with those of propofol and midazolam. Eur J Anaesthesiol 2006;23:1037-40. [PubMed]
17. Taniguchi T, Kidani Y, Kanakura H, et al. Effects of dexmedetomidine on mortality rate and inflammatory responses to endotoxin-induced shock in rats. Crit Care Med 2004;32:1322-6.[PubMed]
18. Nishina K, Akamatsu H, Mikawa K, et al. The inhibitory effects of thiopental, midazolam, and ketamine on human neutrophil functions. Anesth Analg 1998;86:159-65.[PubMed]
19. Clinton LW, Warriner CB, McCormack JP, Alison MC. Reconstituted thiopentone retains its alkalinity without bacterial contamination for up to four weeks. Can J Anaesth 1992;39:504-8.[PubMed]
20. Farrington M, McGinnes J, Matthews I, Park GR. Do infusions of midazolam and propofol pose an infection risk to critically ill patients? Br J Anaesth 1994;72:415-7.[Abstract]
21. Gudmundsson A, Erlendsdottir H, Gottfredsson M, Gudmundsson S. Impact of pH and cationic supplementation on in vitro postantibiotic effect. Antimicrob Agent Chemother 1991;35:2617-24.[PubMed]
22. Roy JJ, Varin F. Physicochemical properties of neuromuscular blocking agents and their impact on the pharmacokinetic-pharmacodynamic relationship. Br J Anaesth 2004;93:241-8.[PubMed]
23. Donati F, Varin F, Ducharme J, et al. Pharmacokinetics and pharmacodynamics of atracurium obtained with arterial and venous blood samples. Clin Pharmacol Therapeut 1991;49:515-22.[PubMed]
24. Dragne A, Varin F, Plaud B, Donati F. Rocuronium pharmacokinetic- pharmacodynamic relationship under propofol and isoflurane anesthesia. Can J Anaesth 2002;49:353-60. [PubMed]
25. Laurin J, Donati F, Nekka F, Varin F. Peripheral link model as an alternative for pharmacokinetic-pharmacodynamic modeling of drugs having a very short elimination half-life. J Pharmacokinet Biopharm 2001;28:7-25.[PubMed]
[TOP]