Samuel Stebbins,1Sean Tackett,2 Charles J. Vukotich, Jr.1
1Center for Public Health Practice, Graduate School of Public Health, University of Pittsburgh, PA; 2Bayview Medical Center, Baltimore MD, USA
Correspondence: Charles J. Vukotich, Jr., Center for Public Health Practice, Graduate School of Public Health, University of Pittsburgh, 130 DeSoto St., A711 Crabtree, Pittsburgh, PA 15261, USA. E-mail: charlesv@pitt.edu
Key words: clerkship, public health, medical education.
Acknowledgements: the authors would like to acknowledge Drs. John Mahoney, Roberta Ness and Bruce Dixon for their leadership in making this applied course possible. We would also like to recognize all of the staff of Allegheny County Health Department and other participating agencies for the many hours that they have spent sharing their expertise and experience with our medical students. This course would not be possible without them. This project was supported by Cooperative Agreement number 5UCI000435-02 from the Centers for Disease Control and Prevention (CDC). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of CDC.
Contributions: CJV full access to all aspects of the research and writing process, and takes final responsibility for the paper; SS and CJV created the curriculum referenced in this article, and participated on all aspects of the research; ST took the course as a medical student and contributed to the background research, analysis and interpretation, and writing of this paper. The authors meet the ICMJE criteria for authorship.
Conflict of interest: the authors report no conflicts of interest.
This manuscript, was previously presented at the 2010 AAMC Conference Patients & Populations: Public Health in Medical Education, has been submitted solely to Medical Education.
Received for publication: 23 November 2010.
Revision received: 19 January 2011.
Accepted for publication: 24 January 2011.
©Copyright S. Stebbins et al., 2011
Licensee PAGEPress, Italy
Medical Education Development 2011; 1:e3
doi:10.4081/med.2011.e3
AbstractAlthough proposals for more public health education go back to 1855, the Institute of Medicine’s (IOM) landmark report, The Future of Public Health (1988) set the modern stage for reform of medical student education regarding public health. The momentum to improve and increase public health education has grown over the last several decades. The authors present the design of a unique public health clerkship for third and fourth year medical students, the Public Health Field Practicum. Students spend four weeks in an integrated program of public/environmental health activities, coupled with weekly didactic and feedback sessions with the course directors. Ten students have completed the practicum since its inception in March 2007. Significant increases in knowledge, desire to include public health in their medical career, and satisfaction are documented. Students gained substantial insight into public health and how it functions in the real world. This training requires a partnership between schools of public health and medicine and local/state health departments. Medical schools should develop these relationships to provide experiential public health opportunities for their students. |
Although proposals for more public health education go back to 1855,1 the Institute of Medicine’s (IOM) landmark report The Future of Public Health (1988)2 set the modern stage for reform of medical student education in public health, and subsequent reports in 20033 and 20074 developed these ideas in more detail. Important stakeholders in medical education have supported this trend, including the American Association of Medical Colleges (AAMC),5 American Medical Association (AMA)6 and American Public Health Association (APHA).7 The Standards for Accreditation of Medical Education Programs (May 2010) now include public health science as a biomedical science in ED-11, which stipulates content that must be included in the curriculum of a medical education program.8 This is a significant advance.
Medical students graduate and become an important part of the Public Health System2 without understanding what it is, their role in it or without ever having set foot in a public health department. Consequently, physicians practice in the community without having been trained in the community, diagnose conditions that have environmental roots and have no contact with environmental health, and work with or for public health or related agencies without previous agency exposure.
Medical students recognize the inadequacy of their training in public health. In the annual graduation questionnaire from AAMC, 30% rated public health training as inadequate. Coverage of public health subcategories of occupational medicine, environmental health, policy, and disaster management were rated inadequate by 40-42% of students.9
The Public Health Field Practicum is one response to this challenge, providing a practice-based clerkship that exposes the student to public health in the real world.
Beginning in 2007, the University of Pittsburgh School of Medicine (UPSOM), in partnership with the Graduate School of Public Health (GSPH) and the Allegheny County Health Department (ACHD), developed the Public Health Field Practicum, a 4 week elective public health clerkship for third and fourth year medical students. The genesis of this course was a convergence of the current course faculty with a movement by UPSOM to improve public health education in the medical curriculum.
The course was designed to highlight the 1988 Institute of Medicine’s core public health functions of assessment, assurance, and policy development.2 In addition, activities were selected to be i) experiential to the greatest extent possible, ii) relevant to the general field of medicine (and thus more likely to intersect with student clinical activities), iii) emphasizing the wide range of public health activities in the broadest possible way, and iv) interlinked with the didactic teaching listed below.
The clerkship provides a hands-on public health experience for students, who spend approximately 80 percent of the four weeks working in the field with a variety of public health professionals and have core and supplementary weekly didactic and feedback sessions with the course directors. The course is designed to emphasize the full range of public health, with special emphasis placed on environmental health which was found in few existing programs in other schools and has a history of being overlooked in medical schools.10 The focus is on integrating the experience into students’ current and future medical training and career.
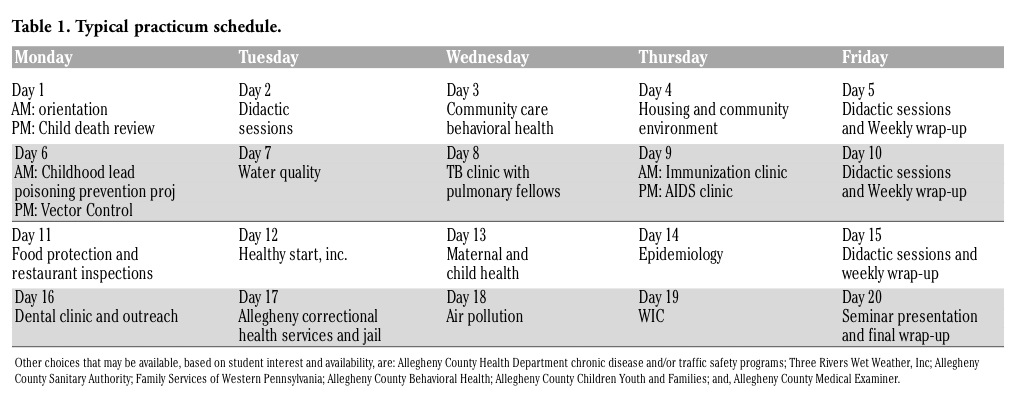
Prior to the beginning of the course, students meet with the course directors to review the curriculum and discuss areas of particular interest. Where possible, the schedule is modified to ensure that the experience includes areas of greatest interest to the student, yet remains comprehensive. Table 1 shows a grid with a typical four week schedule for a student. The field placements ideally involve the student being involved in an activity. Students accompany staff on inspections of restaurants, homes, landfills, etc. They often assist with inspections and have first-hand encounters with rats, roaches and sewage. They assist medical staff in clinic experiences and home visits, where possible. For example, medical students have assisted a dentist at a dental sealant clinic. The opportunity to speak with staff provides important insights, even when a field experience is not possible. Students gain a full appreciation for the work of the doctors, nurses, sanitarians and other public health professionals.
In addition to the field experiences, the students participate in structured didactic sessions on topics which include i) public health practice, ii) causation from a public health perspective, iii) the intersection of clinical medicine and public health and how to use this to your advantage, iv) the legal basis of public health, v) the Ten Essential Public Health Services, vi) the organization of health departments and boards of health, vii) program and strategic planning, viii) the National Public Health Performance Standards, ix) Mobilizing for Action through Planning and Partnerships, x) report and grant writing, and xi) an overview of Allegheny County Health Department’s mission, structure, and function. “Translational science” has become very important in research and medicine; students receive didactic instruction, discussion with course directors, and write a short paper on translational applications based on their own research or experiences.
The biggest challenges have been i) funding for development and ii) difficulty in “repaying” local public health department staff for their time.
|
Table 1. Typical practicum schedule. |
Ten students have completed the practicum (UPSOM catalog # MSELCT 5858) since its inception in March 2007, for an average of 3 per year. Participating students bring varying degrees of previous experience in public health. Two had worked in public health agencies and one already had an MPH. Students have gone on to residency in internal medicine (4), psychiatry (2), pediatrics (2), and emergency medicine (1). One is still in school.
Students create a written evaluation for each individual experience, write a weekly report, and fill out a pre/post learning assessment and overall course evaluation. In addition, at the end of the practicum students create and present a seminar which summarizes their experience, including their observations and insights into how this fits into their medical education and future medical practice.
Student satisfaction with the experience and learning outcomes are high. The students complete a general evaluation of the course and a pre/post learning assessment. On a Likert scale of 1=Poor to 5=Excellent, students rated the course an average of 4.5 overall. All students reported being “more interested” in careers in public health as a result of the experience. Three planned to obtain MPH degrees.
At the beginning and end of the course, students are given a standard pre/post assessment of knowledge. Students are asked about their knowledge/experience of approximately 14 subjects, based on their individual field placements (See Table 1 for typical placements.). These are scored on a 5-point Likert scale of 1=Nothing, 3=Basic Knowledge and 5=Proficient. Collectively there was an increase in each of the 14 areas. Summing all areas, pre/post learning increased from 2.78 to 4.03, or a change of +1.25, which was significant both in scale and statistically (P<0.0001; t-test, assuming unequal variances).
Students may also reflect the success of the program in additional ways. One student wrote an opinion/editorial to the local newspaper in response to criticism of the local health department. His published article stated, in part, “the problem is not that Dr. Bruce Dixon or his staff lacks a commitment to our health; it is that generations of county leaders have failed to make the investments needed to ensure our future safety. I hope that [the county official] will use this as an opportunity to make good on his rhetoric and find the funding our Health Department deserves.”11 Finally, the authors ask the students to describe what is best about this elective and in what ways the course helps them to become physicians better able to integrate public health with medical concepts and roles, and to be a bridge between these disciplines in their future careers. Their responses, shown in Table 2, reflect insight and enlightenment with regard to public health, medicine, and their training as physicians.
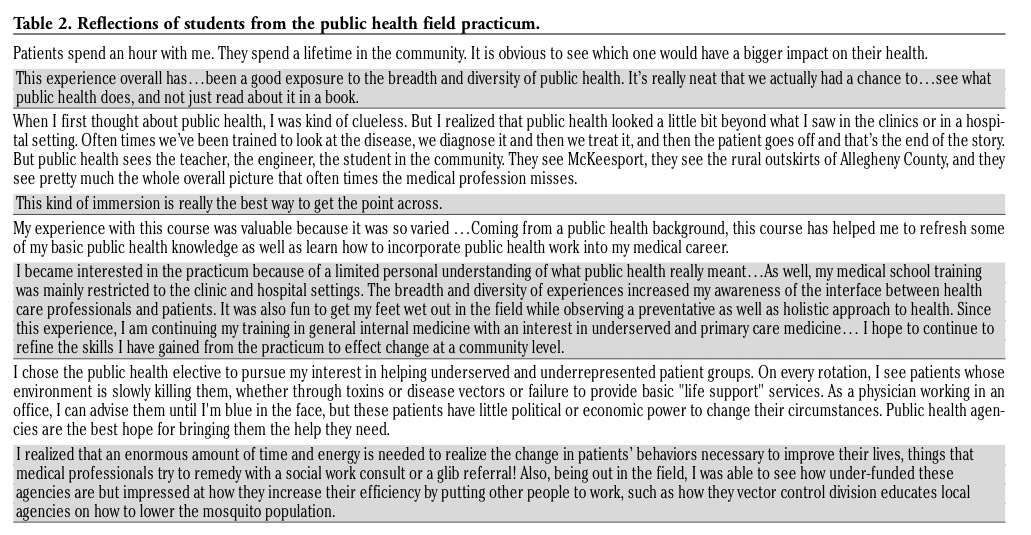 |
Table 2. Reflections of students from the public health field practicum. |
A limitation of these findings is that the students are a self-selected sample. They take the public health clerkship because they are interested, so are more likely to be positive about the outcome. This is reinforced by the reaction of the course mentors, who universally note the enthusiasm and high level of interest of the students. This result is also limited to the United States, Canada and other countries using the Flexner model of medical school education. This course is broad but not deep, and can only represent one component of a comprehension public health education. Finally, it is limited in the number of students because health department and other agency staff can only accommodate a few students at a time in the current structure.
Courses such as the Public Health Field Practicum are essential for medical students. They provide a unique opportunity for students to experience the world of their patients as an essential part of their training. MSELCT 5858 is possible because of an advantageous set of circumstances, with existing connections between UPSOM, GSPH, and ACHD. These relationships are integral to effective functioning of the Public Health System as defined by The National Public Health Performance Standards Program.12 The authors recommend that all medical schools explore the creation of these opportunities and relationships where they do not exist and the development of similar clerkships.
1. Maeshiro, R. Responding to the Challenge: Population Health Education for Physicians. Acad Med 2008;83:319-20.[Pubmed]
2. Institute of Medicine: The Future of Public Health, National Academies Press, Washington DC, 1988.
3. Institute of Medicine: Who will keep the public healthy? Educating health professionals for the 21st century. Washington, DC: National Academies Press, 2003.
4. Institute of Medicine: Training Physicians for Public Health Careers; Washington DC, National Academies Press, 2007.
5. Association of American Medical Colleges, Contemporary Issues in Medicine: Medical Informatics and Population Health, Medical School Objective Project; Washington DC; AAMC, June, 1998.
6. Association of American Medical Colleges and the American Medical Association, Functions and Structure of a Medical School, Washington, DC: AAMC, 1997.
7. Beitsch LM, Brooks RG, Glasser JH, Coble YD. The medicine and public health initiative: Ten years later, Am J Prev Med 2005; 29:149-153. [Pubmed]
8. Functions And Structure Of A Medical School Standards for Accreditation of Medical Education Programs Leading to the M.D. Degree, Liaison Committee on Medical Education, Washington DC/Chicago IL, June 2010, http://www. lcme.org/functions2010jun.pdf, accessed June 15, 2010
9. Association of American Medical Colleges Graduation Questionnaire, http://www. aamc.org/data/gq/allschoolsreports/start.htm accessed 12/21/2009
10. Schwartz BS Rischitelli, Hu H. The future of environmental medicine in Environmental Health Perspectives: where should we be headed? Environ Health Perspect 2005;113;AS74-6.[Pubmed]
11. Widge A. “More Bite Needed.” Pittsburgh Post Gazette, Letters to the Editor. Jan 4, 2009.
12. Local Public Health System Performance Assessment – Model Standards Version 2, CDC, Atlanta Georgia, (standard 10.2) http://www.naccho.org/topics/infrastructure/NPHPSP/upload/FINAL-Local-MS.pdf, accessed July 5, 2010.
[TOP]