Jun Iwamoto,1,2 Tsuyoshi Takeda,1 Yoshihiro Sato,3 Hideo Matsumoto1
1Institute for Integrated Sports Medicine, Keio University School of Medicine, Shinjuku-ku, Tokyo; 2Department of Orthopaedic Surgery, Keiyu Orthopaedic Hospital, Gunma; 3Department of Neurology, Mitate Hospital, Tagawa, Fukuoka, Japan
Correspondence: Jun Iwamoto, Institute for Integrated Sports Medicine, Keio University School of Medicine, 35 Shinanomachi, Shinjuku-ku, Tokyo 160-8582, Japan. E-mail: jiwamoto@sc.itc.keio.ac.jp
Key words: leptin, knee osteoarthritis, interleukin, growth factor, fat mass.
Conflict of interest: the authors report no conflicts of interest.
Received for publication: 4 April 2010.
Revision received: 7 July 2010.
Accepted for publication: 8 July 2010.
©Copyright J. Iwamoto et al., 2010
Licensee PAGEPress, Italy
Rheumatology Reports 2010; 2:e6
doi:10.4081/rr.2010.e6
AbstractAging, obesity, and female gender are risk factors for osteoarthritis (OA) of the knee. Basic research has suggested that leptin may play an important role in the pathological process of OA, and that interleukins (ILs) and growth factors may be related to this process. The objective of the present clinical study was to examine the possible correlations between the serum leptin concentration and gender, fat mass, and the IL and growth factor levels in synovial fluid among patients with knee OA. Forty-four patients with knee OA and hydrarthrosis (age: 50-88 yr) were recruited in our outpatient clinic. Plain radiographs of the knee were taken, and blood and synovial fluid of the knee joint were collected. The serum leptin concentration was significantly higher in women than in men. A simple linear regression analysis showed that body weight, body mass index, and total fat mass, but not age, height, radiographic grade of knee OA, lean body mass, or the levels of IL-6, transforming growth factor-β (TGF-β), or insulin-like growth factor-1 (IGF-1) in synovial fluid were significantly correlated with the serum leptin concentration. A multiple regression analysis showed that among gender and the three above-mentioned significant factors, only gender and total fat mass were significantly associated with the serum leptin concentration. These results suggested that the serum leptin concentration was higher in women than in men and that it was related only to an increased total fat mass in patients with knee OA. However, the present clinical study failed to show a significant correlation between the serum leptin concentration and the IL or growth factor levels in synovial fluid.
|
Leptin, the product of the ob gene, is a peptide hormone that plays an important role in the regulation of body weight by centrally inhibiting food intake and stimulating energy expenditure.1 Leptin is secreted primarily by the adipocytes, enters the circulation, and crosses the blood-brain barrier to reach its primary target, receptors in the hypothalamus. The serum leptin concentration is correlated with the body fat mass2 and acts at the hypothalamic central level as a satiety factor inducing a decrease in food intake and an increase in energy consumption.
Leptin receptors have also been found in articular cartilage, implying a role in leptin synthesis and secretion.3 Leptin has been suggested to play catabolic and anabolic roles in cartilage metabolism and may be involved in the pathological process of osteoarthritis (OA).4 Basic research has suggested that interleukins (ILs) and growth factors may also be related to this process.4,5,6,7 Thus, the serum leptin concentration in patients with OA as well as these other factors could be associated with a risk for OA of the knee.
Aging, obesity, and female gender are risk factors for OA of the knee.8 Knee OA is the most common type of arthritis and the major cause of chronic musculoskeletal pain and mobility disability in elderly populations, representing a significant burden on healthcare provision. Clinically, however, the correlation between the serum leptin concentration and the severity of OA or the IL and growth factor levels has not been fully elucidated. Clarifying the associations between the serum leptin concentration and gender, fat mass, and the IL and growth factor levels in the synovial fluid of patients with knee OA would be of great interest. The objective of the present clinical study was to determine the associations between the serum leptin concentration and various factors including age, height, body weight, body mass index (BMI), lean body mass, total fat mass, radiographic grade of OA, and the IL and growth factor levels in synovial fluid among patients with knee OA.
Japanese patients with OA of the knee and subsequent hydrarthrosis who visited our outpatient clinic (orthopedics and sports medicine clinic) in 2002 or 2003 were recruited. All the patients had consulted experts in knee OA treatment at our clinic because of knee pain. The diagnosis of OA of the knee was made based on the clinical symptoms, the results of a physical examination, and X-ray findings of the knee. All the patients had mild, moderate, or severe OA of the knee (grades 1-4) according to the Kellgren and Lawrence method of grading (grade 0, normal; grade 1, possible osteophytes only; grade 2, definite osteophytes and possible joint-space narrowing; grade 3, moderate osteophytes and/or definite joint-space narrowing; and grade 4, large osteophytes, severe joint-space narrowing, and/or bony sclerosis).9 Because pharmacological treatments such as oral nonsteroidal anti-inflammatory drugs (NSAIDs) and intra-articular injections of hyaluronate sodium are effective for symptom relief,10,11 most of the patients were receiving weekly to monthly intra-articular injections of hyaluronate sodium and/or oral NSAIDs. Comorbidity of the target population included type 2 diabetes (n=2), hypertension (n=5), hyperlipidemia (n=6), gastritis (n=1), cervical or lumbar spondylosis (n=12), spinal scoliosis (n=1), lumbar spinal canal stenosis (n=5), or osteoporosis (n=10, all of the patients were treatment naïve). Type 2 diabetes, hypertension, hyperlipidema, and gastritis were well controlled, and none of the patients had severe obesity and its associated complications such as severe vascular inflammation, severe type 2 diabetes, and severe alteration of lipid and glucose metabolism. None of them had been treated with glucocorticoid, bisphosphonates, estrogen, or other hormones. Thus, the study subjects did not have any comorbidity and treatment (medication) directly affecting the adipocytes that primarily secrete leptin. The assessment of fat mass sets off the conditions indirectly affecting the adipocytes, such as comorbidity, medication, and diet.
One-month after the cessation of intra-articular injections of hyaluronate sodium, dual-energy X-ray absorptiometry (DXA) scanning was performed on the whole body. Serum and synovial fluid were collected from all the patients between 9:00 am and 11:00 am, and the serum leptin and the IL-1α, IL-1β, IL-6, transforming growth factor-β (TGF-β), and insulin-like growth factor-1 (IGF-1) concentrations in the synovial fluid were measured. Then the factors that were correlated with the serum leptin level were determined. Because hyaluronate sodium may affect inflammatory cytokines such as IL-1β and IL-6 in patients with knee OA,12,13 we collected the synovial fluid one-month after cessation of intra-articular injections of hyaluronate sodium. Informed consent was obtained from each patient. This protocol was approved by the Ethics Committee of Keiyu Orthopaedic Hospital.
The serum levels of leptin were measured using a radioimmunoassay (RIA) (normal range: 2.5-21.8 ng/mL). The levels of IL-1α, IL-1β, and TGF-β in the synovial fluid were measured using an enzyme immunoassay (EIA). The levels of IL-6 in the synovial fluid were measured using a chemiluminescent enzyme immunoassay (CLEIA). The levels of IGF-1 in the synovial fluid were measured using an immunoradiometric assay (IRMA).
DXA scanning was performed on the whole body in the supine position using a Norland XR-36 instrument (Norland, Fort Atkison, WI, USA). The lean body mass and total fat mass were measured.
The serum leptin concentration was compared between men and women using an unpaired t-test. A simple linear regression analysis was used to examine possible correlations in the serum leptin level with age, body weight, height, BMI, lean body mass, total fat mass, radiographic grade of knee OA, and the IL and growth factor levels in synovial fluid. A multiple regression analysis was used to determine factors correlated with the serum leptin level among factors that had a significant correlation with the serum leptin level in an unpaired t-test or a simple linear regression analysis. In this analysis, gender was converted to a binary format (men: 0, women: 1). All statistical analyses were performed using the Stat View-J5.0 program on a Windows computer. A significance level of P<0.05 was used for all the comparisons.
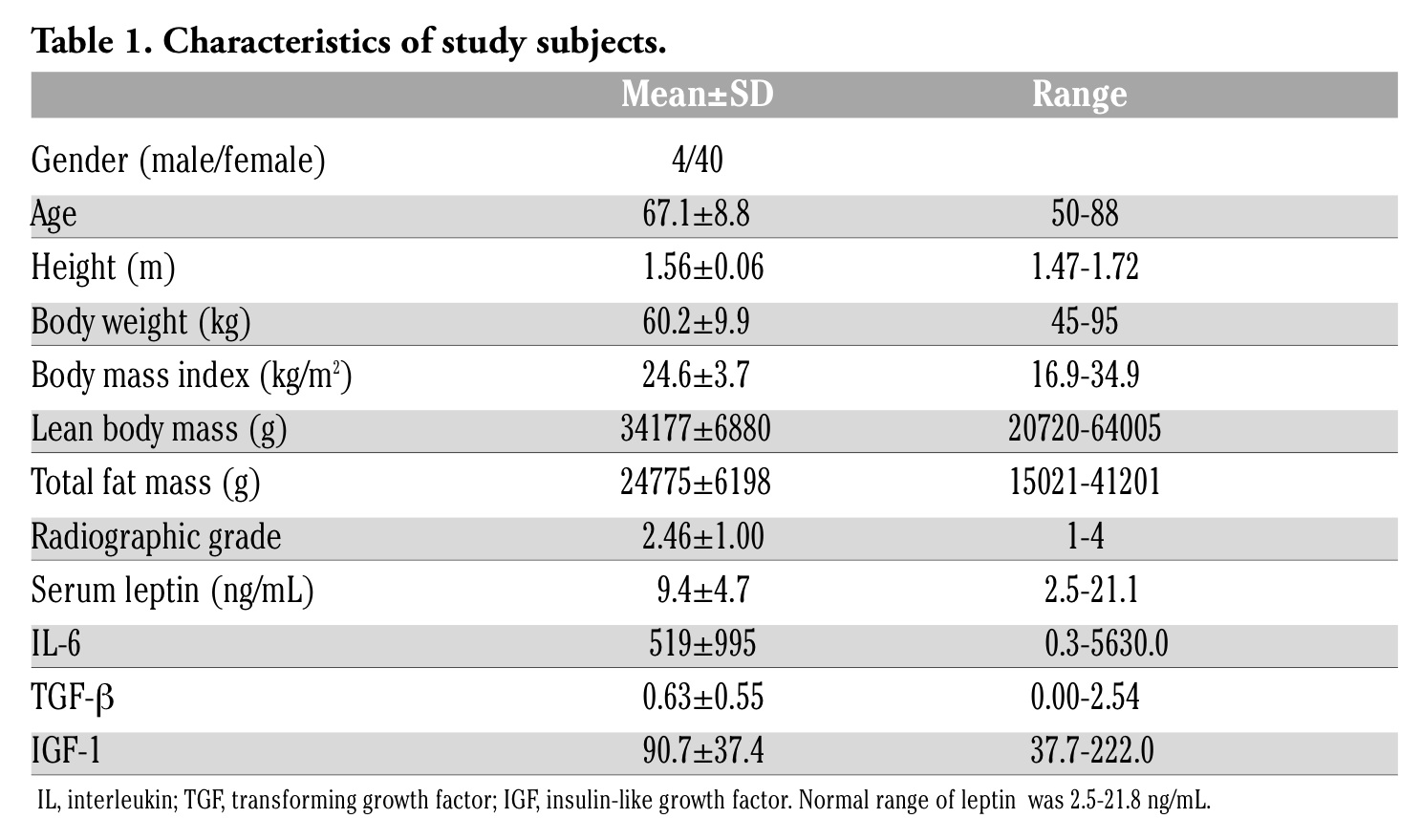
Table 1 shows the characteristics of the study subjects. The mean age was 67.1 years, and the mean BMI was 24.6 kg/m2 (normal range: 18.5-25.0 kg/cm2), corresponding to a “normal-high” level for the Japanese populations. The mean serum leptin level was 9.4 ng/mL (within normal range). Because the levels of IL-1α and IL-1β in synovial fluid were not detected in most of the subjects, these parameters were omitted.
The serum leptin concentration was significantly higher among women than among men (mean value: 9.98 vs. 4.08 ng/mL, Figure 1). A simple linear regression analysis showed that body weight, BMI, and total fat mass, but not age, height, radiographic grade of knee OA, lean body mass, or the IL-6, TGF-β, or IGF-1 levels in synovial fluid, were significantly correlated with the serum leptin level (Table 2). A multiple regression analysis showed that among gender and three factors that were significantly correlated with the serum leptin concentration, only gender and the total fat mass were significantly associated with the serum leptin concentration (r2=0.637, Table 3).
Figure 1 also shows the correlation between the serum leptin level and the total fat mass according to a simple regression analysis.
|
Table 1. Characteristics of study subjects. |
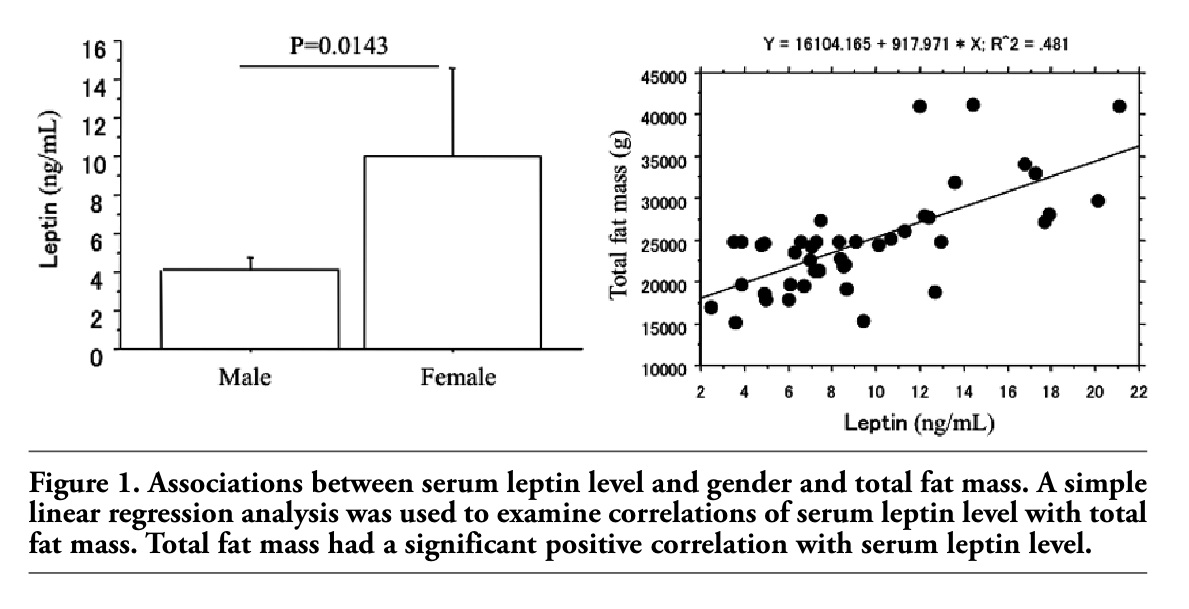 |
Figure 1. Associations between serum leptin level and gender and total fat mass. A simple linear regression analysis was used to examine correlations of serum leptin level with total fat mass. Total fat mass had a significant positive correlation with serum leptin level. |
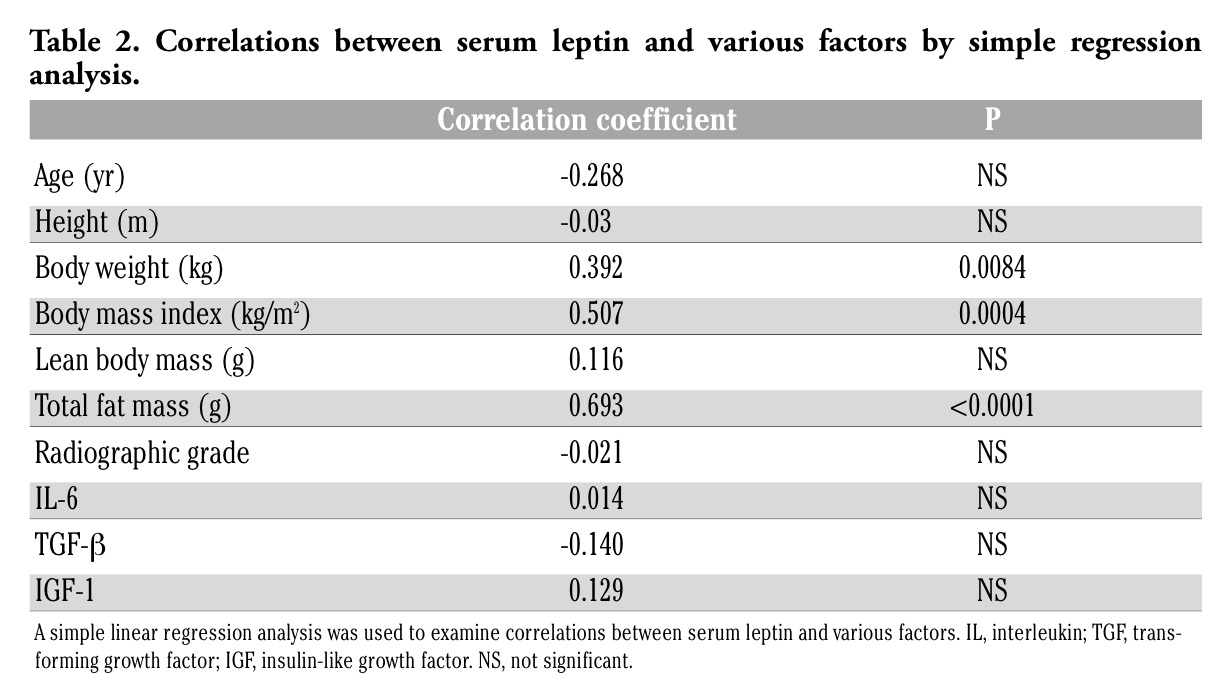 |
Table 2. Correlations between serum leptin and various factors by simple regression analysis. |
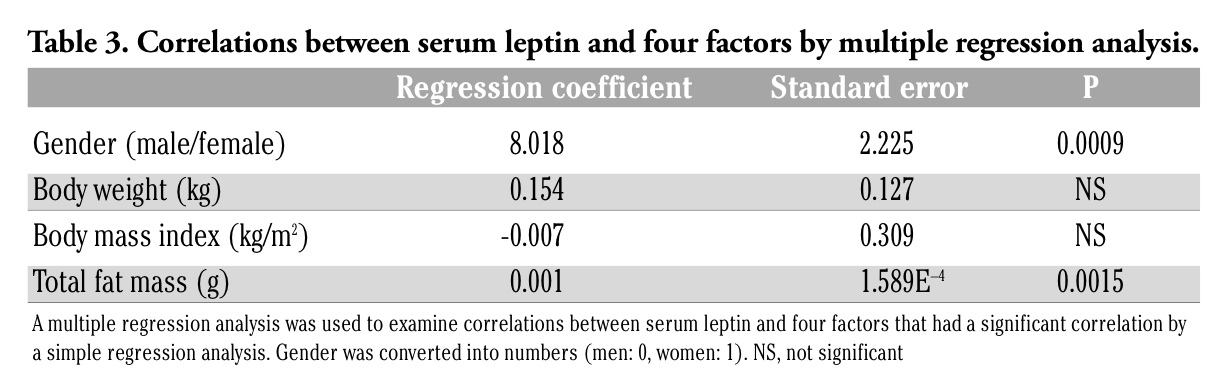 |
Table 3. Correlations between serum leptin and four factors by multiple regression analysis. |
The present study was performed to determine the possible correlations between the serum leptin concentration and various factors including gender, age, height, body weight, BMI, lean body mass, total fat mass, radiographic grade of OA, and the IL and growth factor levels in synovial fluid among patients with knee OA. The results showed that the serum leptin concentration was higher in women than in men and that it was related to an increase in the total fat mass, but not to the IL and growth factor levels in synovial fluid.
Well-established risk factors for OA include aging, obesity, and female gender.8 As a result of the effects of sex hormones, the serum leptin concentration is two- to three-fold higher in women than in men, independent of adiposity, and this difference may be relevant to the influence of gender on the development or frequency of OA.14,15 In our outpatient clinic, the proportion of knee OA patients is about 10-fold higher in women than in men. The serum leptin concentration was 2.45-fold higher in women than in men in the present study.
The serum leptin concentration is known to be very closely correlated with the fat mass, and OA is strongly correlated with a high BMI.16 In the present study, the BMI was normal-high, and the serum leptin concentration was correlated with an increase in the total fat mass. The relationship between obesity and OA is an important public health issue. An experimental study showed that extreme obesity arising from impaired leptin signaling induces alterations in subchondral bone morphology without increasing the incidence of knee OA, suggesting that body fat, in and of itself, might not be a risk factor for joint degeneration.17 Obesity alone does not cause knee OA, but leptin could be involved in OA because without leptin, obesity was not sufficient to predispose an individual to OA.17
Leptin plays a key role in the pathogenesis of OA. Dumond et al.5 reported that leptin strongly stimulates anabolic activity in chondrocytes, inducing the synthesis of IGF-1 and TGF-β at both the mRNA and protein levels. This process may protect cartilage from degeneration in OA, indicating a compensatory protective role during OA pathogenesis. On the other hand, Simopoulou et al.6 reported that leptin enhanced the production of IL-1β, metalloproteinase-9 (MMP-9), and MMP-13 in chondrocytes, indicating a pro-inflammatory and catabolic role of leptin on cartilage metabolism. Bao et al.4 also reported that leptin enhanced the production of catabolic factors, such as MMP-2, MMP-9, and cathepsin D, and down-regulated an anabolic factor, basic fibroblast growth factor (bFGF), in articular cartilage. Furthermore, Distel et al.7 indicated that the infrapatellar fat pad cytokine profile typically found in OA patients could play a role in paracrine inflammation via the local production of the IL-6/sIL-6 receptor, and such a profile might contribute to damage in adjacent cartilage. Thus, leptin may have dual effects on the articular cartilage, and MMPs, ILs, and growth factors may contribute to the pathogenesis of OA.
In the present study, because IL-1α and IL-1β in the synovial fluid were not detected in most of the patients, these parameters were omitted. However, a significant correlation between serum leptin concentration and the severity of knee OA or the IL-6, TGF-β, or IGF-1 levels in synovial fluid was not observed, probably because the values of these parameters varied widely. Clinically, a synovial fluid analysis might not predict the current and future cartilage damage caused by leptin in patients with knee OA. However, Ku et al.18 reported that synovial fluid leptin concentrations were closely related to the radiographic severity of OA. Thus, an evaluation of the leptin concentrations in both synovial fluid and serum as well as the IL and growth factor levels and fat mass might be useful for studying the severity of knee OA. MMPs, cathepsin D, and bFGF were not assessed in the present study. Thus, further studies are needed to clarify the possible associations between the serum leptin concentration and these factors.
The present study has a few limitations. First, a control group was not examined. Therefore, none of the parameters assessed were compared between patients with knee OA and a normal population. Second, the number of study subjects might not have been sufficient to observe significant correlations between the serum leptin concentration and factors other than total fat mass, particularly the radiographic grade of knee OA.
In conclusion, the present study evaluated serum leptin concentration, gender, radio- graphic grade of knee OA, body size, fat mass, and the IL and growth factor levels in Japanese patients with knee OA. The serum leptin concentration was higher in women than in men and was only related to an increase in the total fat mass. However, the present study failed to show any significant correlations between the serum leptin concentration and the IL and growth factor levels in synovial fluid.
1. Zhang Y, Proenca R, Maffei M, et al. Positional cloning of the mouse obese gene and its human homologue. Nature 1994;372:425-32. [PubMed]
2. Considine RV, Sinha MK, Heiman ML, et al. Serum immunoreactive-leptin concentrations in normal-weight and obese humans. N Engl J Med 1996;334:292-5. [PubMed]
3. Teichtahl AJ, Wluka AE, Proietto J, Cicuttini FM. Obesity and the female sex, risk factors for knee osteoarthritis that may be attributable to systemic or local leptin biosynthesis and its cellular effects. Med Hypotheses 2005;65:312-5. [PubMed]
4. Bao JP, Chen WP, Feng J, et al. Leptin plays a catabolic role on articular cartilage. Mol Biol Rep 2009. [Epub ahead of print] [PubMed]
5. Dumond H, Presle N, Terlain B, et al. Evidence for a key role of leptin in osteoarthritis. Arthritis Rheum 2003;48:3118-29. [PubMed]
6. Simopoulou T, Malizos KN, Iliopoulos D, et al. Differential expression of leptin and leptin’s receptor isoform (Ob-Rb) mRNA between advanced and minimally affected osteoarthritic cartilage; effect on cartilage metabolism. Osteoarthritis Cartilage 2007;15:872-83. [PubMed]
7. Distel E, Cadoudal T, Durant S, et al. The infrapatellar fat pad in knee osteoarthritis: an important source of interleukin-6 and its soluble receptor. Arthritis Rheum 2009;60:3374-7. [PubMed]
8. Sowers M. Epidemiology of risk factors for osteoarthritis: systemic factors. Curr Opin Rheumatol 2001;13:447-51. [PubMed]
9. Kellgren JH, Lawrence JS. Radiological assessment of osteoarthritis. Ann Rheum Dis 1957;16:494-520.
10. Felson DT. Clinical practice. Osteoarthritis of the knee. N Engl J Med 2006;354:841-8. [PubMed]
11. Bellamy N, Campbell J, Robinson V, et al. Viscosupplementation for the treatment of osteoarthritis of the knee. Cochrane Database Syst Rev 2006;2:CD005321. [PubMed]
12. Sezgin M, Demirel AC, Karaca C, et al. Does hyaluronan affect inflammatory cytokines in knee osteoarthritis? Rheumatol Int 2005;25:264-9. [PubMed]
13. Waddell DD, Kolomytkin OV, Dunn S, Marino AA. Hyaluronan suppresses IL-1beta-induced metalloproteinase activity from synovial tissue. Clin Orthop Relat Res 2007;465:241-8. [PubMed]
14. Thomas T, Burguera B. Is leptin the link between fat and bone mass? J Bone Miner Res 2002;17:1563-9. [PubMed]
15. Gualillo O. Further evidence for leptin involvement in cartilage homeostases. Osteoarthritis Cartilage 2007;15:857-60. [PubMed]
16. Sandell LJ. Obesity and osteoarthritis: is leptin the link? Arthritis Rheum 2009;60:2858-60. [PubMed]
17. Griffin TM, Huebner JL, Kraus VB, Guilak F. Extreme obesity due to impaired leptin signaling in mice does not cause knee osteoarthritis. Arthritis Rheum 2009;60:2935-44. [PubMed]
18. Ku JH, Lee CK, Joo BS, et al. Correlation of synovial fluid leptin concentrations with the severity of osteoarthritis. Clin Rheumatol 2009;28:1431-5. [PubMed]
[TOP]