
Primary cutaneous adenoid cystic carcinoma of the scalp: dermatosurgical approach with favourable outcome
Accepted: 16 May 2022
HTML: 31
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
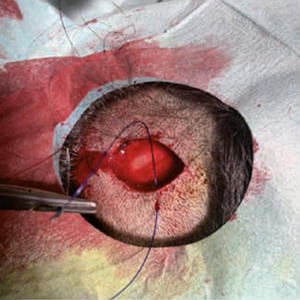
Although described as early as 1975 as a distinct, rare form of cancer with diverse localization, primary cutaneous adenoid cystic carcinoma (PCACC) remains a mystery and challenge for both clinicians and pathologists. The clinical presentation cannot be clearly distinguished from amelanotic melanoma or intradermal nevus, Merkel cell carcinoma, trichofolliculoma, trichoepithelioma or other rare tumors of the adnexa, or dermatofibrosarcoma protuber-ans. The histopathological diagnosis requires not only careful evaluation of standard hematoxylin/eosin preparations, but also immunohistochemical staining with a number of markers such as epithelial membrane antigen (EMA), S-100, SOX-10, Ki-67, CD-117 (c-kit), Vimentin, carcinoembryonic antigen (CEA), Ber-EP4 and many others. The surgical approach should consist of excision with margins between 1 and 2 cm, with the choice of margins depending upon the histopathological findings in the primary excisional specimen. We present a 31-year-old patient with an enlarging, ame-lanotic, plaque-like tumor of the scalp with a duration of no more than 18-24 months. Surgical treatment was performed within two surgical sessions with a total resection field of 1.3 cm. A good cosmetic result was achieved.
Cacchi C, Persechino S, Fidanza L, Bartolazzi A. A primary cutaneous ade-noid-cystic carcinoma in a young woman. Differential diagnosis and cli-nical implications. Rare Tumors 2011; 3:e3. DOI: https://doi.org/10.4081/rt.2011.e3
Naylor E, Sarkar P, Perlis CS, et al. Primary cutaneous adenoid cystic carci-noma. J Am Acad Dermatol 2008;58:636-41. DOI: https://doi.org/10.1016/j.jaad.2007.12.005
van der Kwast TH, Vuzevski VD, Ramaekers F, et al. Primary cutaneous adenoid cystic carcinoma: case report, immunohistochemistry, and review of the literature. Br J Dermatol 1988;118:567-77. DOI: https://doi.org/10.1111/j.1365-2133.1988.tb02469.x
Boggio R. Letter: Adenoid cystic carci-noma of scalp. Arch Dermatol 1975;111:793-4. DOI: https://doi.org/10.1001/archderm.1975.01630180121024
Krishnamurthy A, Vaidhyanathan A. Primary cutaneous adenoid cystic carci-noma of the scalp. Int J Head Neck Surg 2010;1:179-81. DOI: https://doi.org/10.5005/jp-journals-10001-1035
Salzman MJ, Eades E. Primary cutaneous adenoid cystic carcinoma: a case report and review of the literature. Plast Reconstr Surg 1991;88:140-4. DOI: https://doi.org/10.1097/00006534-199107000-00025
Pappo O, Gez E, Craciun I, et al. Growth rate analysis of lung metastases appearing 18 years after resection of cutaneous adenoid cystic carcinoma. Case report and review of the literature. Arch Pathol Lab Med 1992;116:76-9.
Krunic AL, Kim S, Medenica M, et al. Recurrent adenoid cystic carcinoma of the scalp treated with mohs micrographic surgery. Dermatol Surg 2003;29:647-9. DOI: https://doi.org/10.1046/j.1524-4725.2003.29155.x
Numajiri T, Nishino K, Uenaka M. Giant primary cutaneous adenoid cystic carcinoma of the perineum: histological and radiological correlations. Acta Derm Venereol 2008;88:316-8. DOI: https://doi.org/10.2340/00015555-0499
Wick MR, Swanson PE. Primary ade-noid cystic carcinoma of the skin. A clinical, histological, and immunocytochemical comparison with adenoid cystic carcinoma of salivary glands and adenoid basal cell carcinoma. Am J Dermatopathol 1986;8:2-13. DOI: https://doi.org/10.1097/00000372-198602000-00002
Fueston JC, Gloster HM, Mutasim DF. Primary cutaneous adenoid cystic carci-noma: a case report and literature review. Cutis 2006;77:157-60.
Ohtomo R, Mori T, Shibata S, et al. SOX10 is a novel marker of acinus and intercalated duct differentiation in sali-vary gland tumors: a clue to the histogenesis for tumor diagnosis. Mod Pathol 2013;26:1041-50. DOI: https://doi.org/10.1038/modpathol.2013.54
North JP, McCalmont TH, Fehr A, et al. Detection of MYB alterations and other immunohistochemical markers in pri-mary cutaneous adenoid cystic carcinoma. Am J Surg Pathol 2015;39:1347-66. DOI: https://doi.org/10.1097/PAS.0000000000000463
Mohamed A, Gonzalez RS, Lawson D, et al. SOX10 expression in malignant melanoma, carcinoma, and normal tissues. Appl Immunohistochem Mol Morphol 2013;21:506-10. DOI: https://doi.org/10.1097/PAI.0b013e318279bc0a
Terada T. Adenoid cystic carcinoma of the oral cavity: immunohistochemical study of four cases. Int J Clin Exp Pathol 2013;6:932-8.
Matsuba HM, Spector GJ, Thawley SE, et al. Adenoid cystic salivary gland carcinoma. A histopathologic review of treatment failure patterns. Cancer 1986;57:519-24. DOI: https://doi.org/10.1002/1097-0142(19860201)57:3<519::AID-CNCR2820570319>3.0.CO;2-V
Silverman DA, Carlson TP, Khuntia D, et al. Role for postoperative radiation therapy in adenoid cystic carcinoma of the head and neck. Laryngoscope 2004;114:1194-9. DOI: https://doi.org/10.1097/00005537-200407000-00012
Copyright (c) 2022 the Author(s)

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
Downloads
Citations



